
A hysterectomy is a surgical procedure that removes a woman’s uterus or womb. It is a major surgery that has its emotional barriers and challenges.
To better understand this topic, we speak to Dr Chua Peng Teng (MBBS, MOG, AM, FACS), an Obstetrics & Gynaecology Consultant and Surgeon at Mahkota Medical Centre, to shed light on this important topic.

#1: What are the circumstances or conditions in which a woman needs to have a hysterectomy?
Main conditions in which a woman may need to have a hysterectomy (womb removal) can be broadly divided into 2 categories: benign (non-cancerous conditions), malignant (cancerous conditions).
Benign conditions
- It can be due to large mass or tumour from the womb causing difficulty in urination or passing stools (due to said mass causing pressure compression), for example uterine fibroids—which are abnormal growths on the wall of womb. It can grow to large sizes, even occupying the entire abdomen, or grow in multiple numbers.
- Women nearing the menopause age may have more than one disease in the abdomen, for example, large fibroids together with mass in the ovary (female gonad) and when such situation is present, the patient may opt for complete removal of reproductive organs as to reduce the risk or likelihood of the disease coming back again. For young patients who have not completed their family plans however, surgery is usually more conservative and tailored to preserve healthy tissues, hence hysterectomy is not done for this group of patients but rather surgery will aim at removing the disease only.
- Women who have heavy menses, causing distress to their daily lives, and not responding to medications, are candidates for hysterectomy as well. Common diseases that may cause heavy menstrual flow include: uterine fibroids, adenomyosis (swelling of the uterus due to congestion/blood pooling), endometrial polyps (abnormal growth of tissue in the inner lining of the womb), endometrial hyperplasia (overgrowth of inner lining of womb with risk of progressing to uterine or womb cancer).

- A particular condition known as Endometriosis (also called chocolate cyst disease) is an enigma of disease even till today. The common accepted theory is the backflow of menstrual blood into the abdomen causing inflammation and pain. It is also associated with pain during intercourse as well as severe menstrual pains and difficulty to conceive. This condition has a high risk of returning even after conservative treatment or medical treatment. It commonly affects younger women. The dilemma is that although by itself it is not considered cancerous, but as much as 20 percent of cases are associated with ovarian cancer and it behaves in a manner similar to women’s cancer (invading tissues, causing widespread implants and difficult to treat).
- Other causes can be prolapsed organs (uterovaginal prolapse) due to ageing or high number of child births resulting in lax organ supports for the womb (female organs drop down through the vagina due to laxity in the tissues).
Cancer/Malignant conditions:
Removal of the womb is often necessary for cancer of the uterus (womb), ovaries (gonads), cervix (entry /neck of the womb), fallopian tubes, pelvic peritoneum (inner covering of the lower abdomen around the female reproductive organs).
It is important to note that early treatment at stage 0 or stage 1 of the disease carries good survival outcome in most cases. However, most cancer conditions are ‘silent killers’ and it is common for a patient to experience no pain and minimal symptoms and hence they often present at late stage to the doctor’s clinic.
Hysterectomy for cancer conditions or in some cases non-cancer conditions that are difficult to treat (e.g. endometriosis) are usually radical in the sense that more tissue removal around the organ affected is warranted, and mostly require removal of lymphatic tissues or other adjacent organs for complete assessment (staging) of the disease.
In cases of advanced cancers, hysterectomy can also be done as a measure to improve quality of life (palliation hysterectomy). This is done to reduce the disease load or burden for the patient.
#2: What are the benefits and disadvantages of uterus removal?
Benefits of hysterectomy or womb removal:
For non-cancer conditions, it is a means of achieving total removal of disease and although return of disease is possible, it is usually rare and serves as a cure for patient.
For cancer conditions, removal of the womb that is affected would achieve similar purpose of reduction of risk of disease recurring (returning) and may improve response to chemotherapy or radiotherapy. In early stage cancer, a good outcome is possible, whereby a complete removal would only necessitate follow up and patient is spared from the side effect of chemotherapy or other forms of advanced cancer treatment. But this is not always possible as patients often see the doctor very late for their issues. Womb removal also will provide permanent relief for troublesome menstrual problems that do not respond to medical or conservative treatments.
Disadvantages of womb removal/hysterectomy:

Patients need to undergo detailed counselling since there is a risk of regret of one losing the reproductive organs. For older patients who are near the age of menopause, total removal of the womb may not affect the patient much, as in a woman’s natural life cycle, average age of menopause is at 51.
If the patient is young, however, removal of the womb will cause cessation of menses, and inability to conceive, hence a meticulous review of the indication will be discussed with the attending doctor before proceeding with surgery.
#3: What are the long term risks and side effects of not having a womb?
Usually, before removing the womb (hysterectomy), doctors will discuss with patients whether or not the ovaries (female gonads) are to be left behind. If a total hysterectomy includes removing the ovaries, the patient will experience menopause after operation (regardless of age). This is known as a ‘surgical menopause’. With the uterus removed, there is no longer periods—to women, this is something that needs adjustment to.
For younger patients who do not have disease in the ovaries can opt for retention of her ovaries since even after menopause, the ovaries still release testosterone that is responsible for sexual drive in women as well as small amounts of hormone estrogen.
However, studies have shown that women after hysterectomy with retention of both ovaries reached menopause 3.7 years earlier than women who did not have a hysterectomy. Women with one ovary removed at the time of hysterectomy reached menopause 4.4 years earlier than women who had both ovaries left in at the time of hysterectomy. This is potentially due to blood supply changes to the ovaries after removing a major organ such as a womb.

Women who experience natural or surgical menopause will have a lack of estrogen that causes menopausal symptoms such as:
- hot flushes
- depression
- vaginal dryness
- sleep problems (insomnia)
- fatigue
- night sweats
For such cases, some women may require hormone replacement therapy (HRT) to help with menopausal symptoms. Lack of estrogen resulting from removal of ovaries has been associated with higher risks of heart disease, stroke, hip fracture, Parkinsonism, dementia, cognitive impairment, depression, and anxiety.
It is worth noting, however, that removal of ovaries may help reduce risks of breast cancer and ovarian cancer in high risk groups (with known genetic mutations that increase the risk of ovarian and breast cancer i.e. BRCA1 or BRCA2 mutations).
These patients should strongly consider oophorectomy (removal of ovary or both ovaries) following childbearing. Removing the ovaries also prevents future ovarian surgery for ovarian disease.
Usually, hysterectomy (womb removal only) does not cause an increase in heart disease or other chronic diseases.
This is because for hysterectomy, the ovaries/female gonads responsible for hormone production is left behind. Usually the doctor will discuss with the patient whether or not to remove the ovaries together with the hysterectomy procedure. Removing the ovaries will cause stoppage of hormone production and as a result, exposes the woman to risks of menopause such as heart disease, fractures, stroke, mood changes and sexual function changes.
In theory, hysterectomy may cause weakening of the supports of the muscle/tissues in the female pelvis (the female basin-like bone structure containing all the vital reproductive organs) and may result in dropping of organs into the vagina (prolapse). This is however not clearly proven in studies and remain controversial.
#4: How does a woman’s body change after a hysterectomy?
After hysterectomy, a woman will not have her periods and will lose the organ needed for pregnancy. Other than that a hysterectomy generally does not cause change in body image.
#5: Will this affect a woman’s sexual life?

Studies showed unchanged or improved sexual function within 1 to 2 years after surgery. This is likely due to the disease being removed together with the womb. Since only the womb is removed and the hormones produced by ovaries are still on-going, vaginal dryness is usually not an issue.
#6: Is weight gain a consequence of hysterectomy?
To date, it remains controversial whether or not hysterectomy predisposes a woman to weight gain. A direct causal relationship cannot be proven due to many factors involved, such as the woman’s diet habits, daily exercise routines, as well as hormonal status and some medications may all play a part. Weight gain is more likely due to hormonal and dietary habits.
#7: Can you briefly explain the difference between the types of hysterectomy surgery?

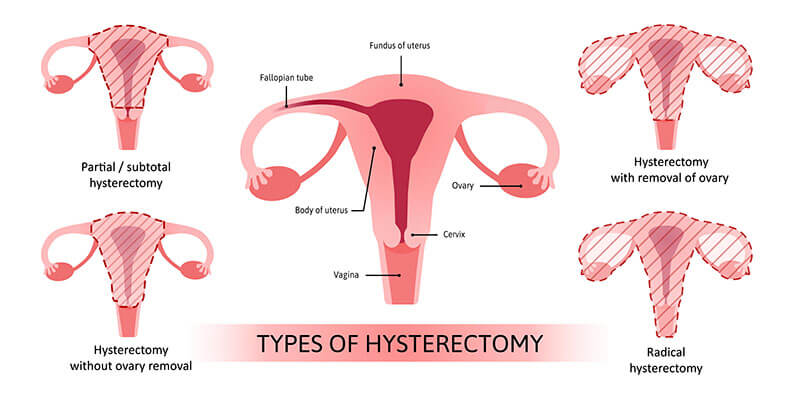
Hysterectomy surgeries can be broadly classified based on approach into:
- laparotomy (open), minimally invasive (keyhole) surgeries,
- for minimally invasive (keyhole) approach, it is further divided into:
- single port (single opening made on abdomen only),
- conventional multiple port (multiple small openings made on abdomen),
- Laparoscopic assisted vaginal (combining keyhole surgery on abdomen and removing the womb from vagina),
- robotic assisted, and
- VNOTES (vaginal natural orifice transluminal endoscopic surgery – a single opening is made in the vagina and keyhole surgery is performed from below, rendering the abdomen totally scarless).
- Vaginal Hysterectomy: Hysterectomy can also be done for dropping of organs (prolapse) due to old age, lax tissues or high number of delivery of babies. This is done through the vagina – called vaginal hysterectomy.
- If a hysterectomy removes the womb together with the cervix (entry of womb) it is known as complete/total. If the hysterectomy does not remove the cervix, it is called Subtotal/supracervical (means only the womb above the cervix is removed).
Diseases like cancer or those that invades surrounding tissues may need removal of more tissues and areas of spread: this is called the radical hysterectomy.
#8: What is the common type opted for?
The type of hysterectomy will be tailored based on individual patient conditions.
#9: What’s the recovery period like, and the dos and don’ts post-surgery?

Recovery is generally faster and shorter with minimally invasive approaches. Patient usually experiences less pain as well as requiring less pain killers. In some cases, patient is fit to go home within 1 or 2 days. This is due to small skin openings and less discomfort from the small incision. Patients generally feel more confident after minimally invasive surgery as they perceive a small skin wound to be easier to take care of.
For any form of tissue injury to fully recover however, will take any time from 2 weeks to 6 weeks. If an open surgery was performed, ward stays can range from 3 to 7 days depending on the case, but again the tissue recovery period is roughly the same. Skin recovery is usually faster after minimally invasive procedures.
As for Dos and Don’ts after surgery, it is important to have a balanced healthy diet comprising of proteins, fibre and vitamins for better tissue recovery and to avoid risks of food poisoning form seafood since this may impair wound healing.
For patients with multiple medical problems like diabetes and hypertension, it is important to ensure that regular medicines are taken since poor control for these chronic diseases will also affect wound healing and recovery. Usually, doctors will advise patients to avoid sexual intercourse or straining and heavy lifting for 6 weeks after surgery since this may cause the sutures or wound to grow weaker due to pressure.
Source: Dr Chua Peng Teng, an Obstetrics & Gynaecology Consultant and Surgeon at Mahkota Medical Centre
Disclaimer: The information provided in this article is for informational purposes only and should not be considered as medical advice from Motherhood. For any health-related concerns, it is advisable to consult with a qualified healthcare professional or medical practitioner.
For more insightful stories and fun recipes, stay tuned to Motherhood Story!