
There comes a time in our life where we plan to grow our family. In recent years, late pregnancy (around late 30’s to 40’s) is a more frequent choice for women to plan on their pregnancy.
However, whether it’s early or late pregnancy both options have their own risks, from the well-being of the baby to how late you can plan for your pregnancy there are many questions afloat!
As things stand, AskMeDoctor!, a weekly Q&A program from Motherhood has invited Dr. Tan Cheng an Obstetrician & Gynaecologist of Tung Shin Hospital to shed some light on today’s topic – Young VS Late Pregnancies.
So, pay attention and get your vilified facts here.
Q1: Does age affect fertility?
Dr. Tan Cheng: We will start from the very beginning. As we know that women/females’ have ovaries. And an ovary is the place where oocytes (which is known as eggs) are formed. So at birth, a female ovary contains roughly about 1–2 million eggs. When you reach puberty, you only have about 25% of them remain.
Let’s say roughly about 300,000. Now one thing to remember is in general, females do not make new eggs. And whatever you were born with, the numbers will just decline continuously throughout the years. Over the next 30 to 40 years, the entire egg supply will be depleted, which is when women reach menopause.


One thing to remember is that 1–2 million oocytes sound like a lot. But by puberty there is only 25% left: 300,000 also, sounds like a lot. But you have to understand that not every of these eggs will reach full maturity. So generally speaking, (roughly) only about 300–500 of these eggs will reach maturity throughout your entire life span.
Q2: So, how does age affect pregnancy?
Dr. Tan Cheng: We can start by talking about when the female is very young. Teenage pregnancy vs. the standard age vs. elderly mother (advanced maternal age).
-
Teenage pregnancy
When they look at teenage pregnancy, they found that if you are between 13 and 16 years old, your pregnancy risks are much higher. The risks include:
- premature delivery
- a small baby
- baby with low birth weight
And because the suggestion is that during this period, a teenager’s body is still growing, the mother requires nutrients to grow. There is a competition between the mother and baby fighting for these nutrients.
They have also found out that babies will have higher mortality. And because the nutrients are in place, teenage pregnancy will have a higher risk of anemia.
There are other complications aw well because we know that the mother is still growing. The pelvis is still immature and small, so there is a higher chance of obstructed labour, which means the baby may not be that easy to deliver normally.
We do not encourage pre-teen pregnancy because you might be fighting for nutrients with your baby. And because you are going through puberty, you are still growing and you need more nutrients.
And your baby, at the same time, needs nutrients to grow as well. So that is for teenage pregnancy.
-
Elderly mother (advanced maternal age)
And now, we are looking at a very advanced age. Not to say very advanced age, but advanced maternal age. They label mothers as advanced maternal age after the age of 35. When we are older, we have a higher chance of getting high blood pressure and diabetes.
Same thing as well, when you are older and you are pregnant, pregnancy risks are also higher. As your age advances, you will have a higher chance of having hypertension, diabetes, smaller babies and premature births as well.
And the most important thing to realise is that the risk of birth defects increases when you are older.

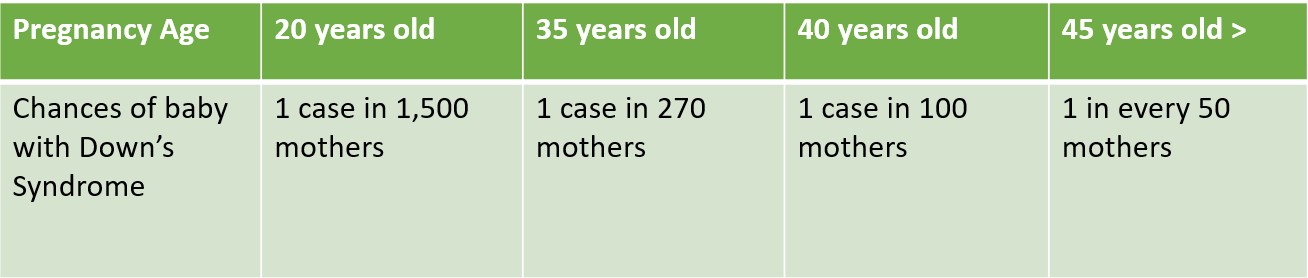
If you are looking at the age of 20 years old, for 1 mother to have a Down’s syndrome baby, there would be only 1 case in 1,500 mothers. But when you hit 35 years old, it is roughly about every 270 mothers, there will be 1 mother with a Down’s syndrome baby.
Once you are 40 years old, it is in every 100 mothers, there will be 1 Down’s syndrome baby. And when you are 45 years old and above, it is more than 1 in every 50 mothers. As your age advances, the risk of birth defects will be higher; the complications are also higher.
Q3: What is the perfect age to have a baby?
Dr. Tan Cheng: The perfect age to have a baby is never during your teenage years. And you will need time for your body to grow and have sufficient nutrients. Also, we advise not to be at a very advanced maternal age as well. Between 20 and 35 years old will be a rough suggestion.
Q4: And how old is too old to get pregnant?
Dr. Tan Cheng: If you are just looking at getting pregnant,there is a possibility until you hit menopause. Anytime before you hit menopause, you are still likely to get pregnant. It is just the risks associated with it will gradually increase as you age.
Q5: What is the average age of women to reach menopause?
Dr. Tan Cheng: It depends on the population, but we are looking at roughly between the age of 45 and 55 years old. This is the age range we see in the general population.
Q6: If I am pregnant with my first born after the age of 35 to 45, what are the things I should take note of?
Dr. Tan Cheng: As long as you are menstruating, you can get pregnant. The risks will keep getting higher as we age. Like you mentioned just now, if I am at the age of 35, what are the things I have to take note of compared to when I am younger?
The things we mentioned previously are the risks associated with age, especially the risks of birth defects and Down’s syndrome. When you reach the age of 35 and you are pregnant, you may start considering antenatal screening.
Antenatal screening comes in a few forms. One of them is ultrasound to look at the nuchal translucency, which is the thickness of the neck of a baby. This is normally done between 11 and 14 weeks.
Through this, it will give a rough idea of what the risks are associated with Down’s syndrome.


And together with a blood test, which is a serum blood test to look at the biochemistry profiles. This is known as the first-trimester screening. It gives you an idea on calculated risks of how likely you are to have a baby with Down’s syndrome.
Some mothers may find out that they are pregnant much later on, which means beyond 14 weeks or maybe in the second trimester. There are also different sets of blood tests. And one of them is known as the triple test or quadruple test.
This is also to look at the serum biochemistry profiles and give you a calculated risk of the likelihood of you having a baby with Down’s syndrome.
Now the latest test that everyone is talking about right now is the non-invasive prenatal testing.
This test can be done when you are 10 weeks pregnant, which is 2½ months. This test is to extract the baby’s genetic materials from the mother’s blood and use that to take a closer look at the baby’s chromosomes.
While looking at Down’s syndrome itself, the accuracy can be as high as 99.4%. This is for the birth defects. As we age, you will have a higher risk of getting diabetes and also, a higher risk of getting high blood pressure.
Every time when you come for a check-up, we will measure your blood pressure. And when you are 28 weeks pregnant, we will do a glucose tolerance test to check for diabetes.
Q7: 3 miscarriages in a row and already in her mid-30s. Is there any chance that at this time it could be a healthy pregnancy with a healthy baby? If yes, what are the chances like?
Dr. Tan Cheng: I am assuming that these three miscarriages have been managed by an obstetrician and gynaecologist. If you have three miscarriages in a row, I am sure that a few tests would have been carried out for you.
There are many causes of it. But the majority of the causes are unknown. All the tests that were conducted is to find that one cause that can be explained and consequently the suitable treatment for that particular cause. So, as to prevent further miscarriages.
-
Antiphospholipid Syndrome (APS)
Now one thing that is possible to diagnose and possible to treat is APS. In this syndrome, they will normally take a blood test to look for the antiphospholipid antibodies, such as lupus anticoagulants and anticardiolipin antibodies.
If these are detected and you have experienced pregnancy loss, then your doctors would advise that you would most likely need to undergo treatments when you are pregnant.
-
Other causes and subsequent treatments:
Now another thing to think about is that if a mother were to have any other underlying diseases, such as hypothyroidism or hyperthyroidism, normally, the thyroid function tests will be conducted as well. Now this is looking at the hormones and looking at the underlying symptoms.
Sometimes a mother may have an abnormally-formed uterus. The doctors will normally do an ultrasound, both transabdominal or transvaginal, to look at the shape of the uterus.
If there is any suspicion that the uterus is not in a normal shape, they may carry out an MRI to get a closer look at the abnormalities.
Another thing that can be considered when you have a miscarriage is the products of conception that have passed. We can potentially send them for psychogenetic testing.
Which tests the genetic materials of the baby to see if there is any syndrome that is causing the miscarriage. If that is identified, then we can start screening both parents to see if there is any genetic abnormality.
Q8: If a woman is pregnant again 2 months after delivering her 1st baby, does becoming pregnant too soon put risk on her or the baby?
Dr. Tan Cheng: Getting pregnant in 2 months after delivering her 1st baby, it depends…
If the first one is a normal vaginal delivery, yes, it is definitely a higher risk because your body has not fully recovered yet. And when you deliver the baby, you will lose some blood and your body will need some time to regenerate the red blood cells.
When we say that it is less than 6 months between your delivery and your next pregnancy, that will require a very short interdelivery interval. It is associated with high risks of anemia, preterm labour, smaller babies and miscarriages as well.
Now let’s say if you have your first child by caesarean section, we will normally advise to wait for 2 years before you get pregnant again. And your wound and uterus need time to heal.

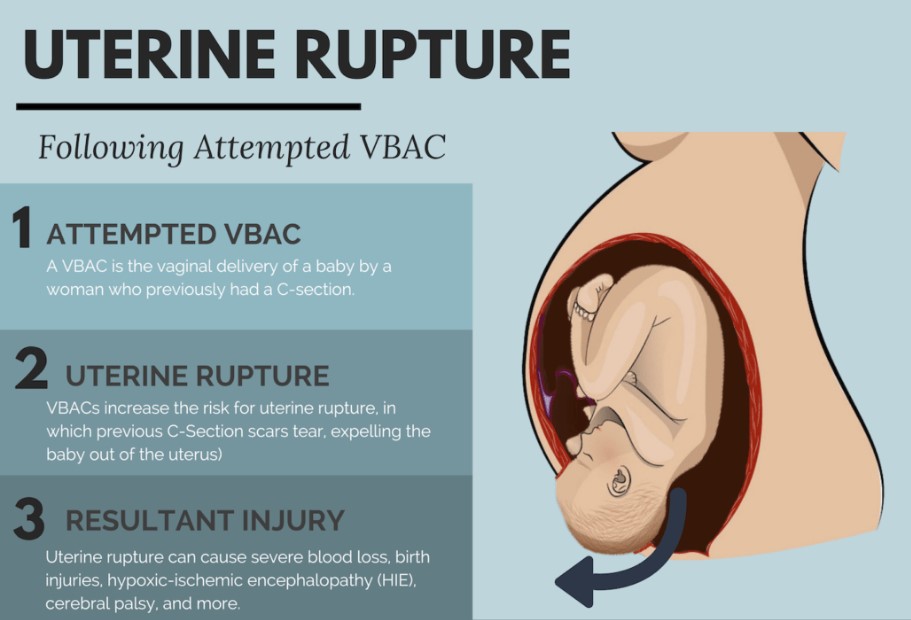
If you are pregnant so soon, your next pregnancy will carry a much higher risk of uterine rupture or uterine dehiscence when your baby is about to be born.
Moreover, when you are about to give birth and if you had a very recent caesarean section, the scar may not be fully healed and you will stand a much higher chance of uterine rupture during the process. So, it is quite dangerous.
Q9. It depends if her first pregnancy is vaginal birth or caesarean delivery?
Dr. Tan Cheng: Yes, if your last cesarean section is not too long ago, we don’t recommend vaginal birth. We recommend a repeat caesarean section because the risk of uterine rupture is higher. Either vaginal birth or caesarean section, we generally advise to wait for 2 years.
For the caesarean section, it should allow time for the wound to heal. And as for vaginal birth, a few reasons why: for your body to recover and also, for your mental health as well so that at least, your first baby is slightly bigger before you have another smaller baby.
After your first pregnancy delivery, you should rest for about 2 years before your second pregnancy.

Q10. If a woman gets pregnant at the age of 20, will the baby be born with a disability?
Dr. Tan Cheng: If you are looking at the literature, the articles, most of the adverse outcomes are actually associated with teenage pregnancy around 13 to 16 years of age. So, it is much earlier than that.
When the body is not fully developed yet, that is when things can go wrong. As I have mentioned previously, premature delivery is higher.
And they found out that for those who delivered before 32 weeks of gestation is highest among the age between 13 and 16 years old.
Babies will tend to be smaller than they are supposed to be and have lower birth weight because the mother is competing for nutrients with the baby. Babies born will have a higher risk of mortality.
Mothers will have a higher risk of anemia and also, a much higher likelihood of obstructed labour, which means difficulty in giving birth as the pelvis may still be immature.
As they are still young, after delivery, they will have a higher chance of experiencing postnatal depression. And sometimes, it is difficult for them to sustain breastfeeding.
Q11. Is it true that if a woman constantly experiences period pain, it will be easier for her to give birth? Will period pain disappear after childbirth?
Dr. Tan Cheng: The first thing is to identify what the cause is of the period pain.
I think most of them are interested in the period pain that is caused by a condition known as endometriosis. Endometriosis is very sensitive to hormones.
When you are pregnant, the hormones that are released during pregnancy may actually suppress the menstrual cycle and alleviate the symptoms. When they are pregnant, they feel that the pain is much better. However, it doesn’t mean the pregnancy cures the period pain and endometriosis.
It will come back after giving birth. When the menstrual cycle has returned, the pain may slowly come back. This is one of the reasons and it is actually one of the most commonly asked questions as well. There is a myth on whether pregnancy itself can cure endometriosis.
Q12. Is it true that giving birth the second time around is easier compared to the first one?
Dr. Tan Cheng: If we’re only looking at just the delivery part…
If the first pregnancy is a vaginal delivery, then yes, the subsequent vaginal delivery will be easier for the mother. But if your first pregnancy is a cesarean section and your second one is a vaginal birth delivery, then it won’t be any easier in comparison because it is the first time the baby is going through the vagina canal.
Q13. Can a woman have cesarean more than once?
Dr. Tan Cheng: The answer is yes for that. If your first cesarean section experience is uneventful and there are no complications, and you have enough inter-delivery intervals, say 2 years of rest before you get pregnant again. For subsequent delivery, you can try normal vaginal delivery.
The success rate is actually quite high, about 72%–75% of mothers with previous cesarean sections can deliver via vaginal birth.
If they manage to deliver via vaginal birth, then for the 3rd, 4th, 5th pregnancy, they can still deliver via vaginal birth again. And there is no limit on how many babies you can have.
But, if let’s say that the first one is cesarean section and the second one is also cesarean section, we generally advise that 3 cesarean sections should end around there.


There is no absolute number of how many cesarean sections you can have, but generally speaking, the more cesarean sections you have, the higher the risk will be on your next pregnancy.
Which is why we generally advise that if you have already had 3 cesarean sections, then maybe it is time for you to consider whether you still want to take the risk to have another one afterwards.
Q14. How do women with scoliosis manage pregnancy and childbirth differently?
Dr. Tan Cheng: Well, it is a very specific question, but unfortunately, we need more details. Scoliosis is actually a range. Some will just have a mild scoliosis, some scoliosis conditions may be very serious.
So, it depends on the severity itself, then the answer will be completely different. Normally, it is a joint discussion between bone doctors, orthopaedics, and also obstetricians. Everyone will have to sit down and discuss the case, and it will be an individualised approach, depending on the severity of the scoliosis.
Q15. Before we end our interview today, do you have any advice for pregnant women?
Dr.Tan Cheng: What I can advise is that everyone is different, so there is no one rule that is fixed for everyone. Every pregnancy, we will have to access it individually, and to find out the best plan that is tailored to you.
So, the best thing to do is actually to discuss with your obstetrician and go through your history because everyone is different; everyone will have different ways and advice. The whole pregnancy journey will be managed differently as well.
Alright folks, that is all for our Week 2 AskMeDoctor!. I’m sure there’s a lot for you to think about after this week’s section. As Dr. Tan has said there is no one size fits all solutions for every mothers out there. Stay tuned for more advices from renowned sources.